This month’s Evidence-Based Parenting Blog Carnival is discussing the transition to motherhood/fatherhood, inspired by Mother’s Day. Our host this month is evidence-based parent Jessica Smock whose blog, School of Smock, looks at parenting from the perspective of a mom with a young child and a research background. Our topics in this month’s carnival are as varied as you might expect. You can find them all here. You can also follow the discussion on Twitter with the hashtag #parentscience and on our Facebook page. Also, tune in on Twitter this Friday (5/17/13) from 1 to 2pm for a Twitter party with all of our bloggers for a live discussion with the hashtag #parentscience.

Last Mother’s Day was my due date with Nemo, my second offspring. I was somewhat impatiently awaiting his arrival. I must say, the transition from one kid to two was a lot easier than the transition to being a new mom. Some of that was due to a more difficult delivery with my first and some of it was due to the amount of help I had with my second (Mac was home with me). However, I think largely it was due to the fact that childcare was already routine. I was used to being woken up in the night. I was used to breast feeding. I was used to diapers and swaddling and baby monitors and naps and sleep deprivation. I’d been there, done that (or in some cases like diapers was still doing it with Mabel) when Nemo came along. Caring for a baby wasn’t new, it was familiar. It was habit.

Meeting Mabel face to face for the first time.
My practical advice to new moms, based on empirical evidence of having been one myself, consists of two things:
1. Keep your expectations low. (That includes expectations of yourself, your baby, and your partner.)
2. Give it about a month before anything feels normal again.
I’ve written about #1 before, here. In all truth, in the early days of parenting, it’s completely necessary and sufficient to just get by. Your house doesn’t have to be clean. Your clothes don’t have to be clean. Your hair doesn’t have to be clean. This study would indicate that you are not alone- 40% of women reported at 1 month postpartum that there were days they did not get dressed. This was my experience too. You can extrapolate from there.
At first, you just get by. When it’s a struggle to just get all living beings in your household fed and clothed, you need to keep your priorities in order. Now having had baby #2, I look back to how I did things with Mabel (#1) and feel like I need to apologize for my ineptitude. We really were just getting by. Learning as we bumbled along.
Why are these early days so hard? I know my fellow EBBs (Evidence-based bloggers) are covering some of that. There’s the sleep deprivation. There might be postpartum depression. You may be learning to breastfeed or struggling to breastfeed. Bonding with the new baby.
I’ve written before about my recoveries (I had a C-section with both kids) in the past. It’s definitely a transition physically, emotionally, and psychologically.

Meeting Nemo face to face for the first time.
When I had my first child, Mabel, I didn’t feel myself for weeks. I felt kind of out of place and on edge. Crawling into bed at night wasn’t a welcome rest, merely a short reprieve. I couldn’t relax and enjoy the rest because I knew, at any moment, it would be interrupted by a crying baby. That getting into/out of bed or rolling over was still painful and I was waking up drenched in sweat each night didn’t add to any sense of rest or relaxation.
My experience is pretty typical if you look at the data. Maloni et al looked at the postpartum symptoms reported by 106 postpartum women who had a singleton high-risk pregnancy and were treated with antepartum (before giving birth) bed rest. At 6 weeks postpartum, at least 40% of the women were still reporting symptoms like fatigue, mood changes, tenseness, and difficulty concentrating. In this particular study, the authors didn’t include any kind of “control” group of women (i.e. those who had not been on bed rest, those that had low risk pregnancies, etc.). If they had included such a group, I would not be surprised if the results were similar. My own anecdotal evidence would indicate that fatigue, mood changes, tenseness, and difficulty concentrating are pretty universal for women after giving birth.
I kind of trudged through the days (and nights) like a zombie- lack of sleep, lack of food (it was hard to find time to eat while caring for a newborn solo), C-section pain, pain medication- the combo wasn’t conducive to coherent thought. Watching the 2010 Winter Olympics is how I kept from slumping over while nursing in the dead of night (perk- I actually got to watch some of it live).
It also didn’t really help that during that time Mabel was lacking in the personality department. It was kind of like caring for a slobbery, leaky, screaming sack of sugar. Her first smile- right around the one month mark was kind of a turning point. She was interactive and that helped with nurturing and caring for her. Also, I think we kind of found our groove. After a month of muddling along, I figured out how to live as a mom, and she figured out how to live outside of my womb.

First family photo a few hours after Nemo was born.
Have you ever heard somebody say it takes 30 days to make a new behavior into a habit? Well, it turns out that there is some science to back up that notion- that it takes time for new behaviors to become habits, to become acclimated to new situations.
So is 30 days some kind of magic threshold? I don’t think so.
By that one month mark, I was able to feel more relaxed at bed time, it no longer felt like there was a stranger in my house, I felt much less tense and on edge. I still wasn’t ‘normal’- the house was still messy, I still spent days in my PJs, but they felt more like a lazy Saturday than futile struggle for self-care.
A few years ago, a group at the University College London, led by Phillipippa Lally studied 96 people who wanted to form a new habit (the article is behind a paywall, but you can find the abstract here). Lally et al looked at how long it took individuals to report that the new behavior had become automatic- basically, had become habit. They found a wide range (from 18 to 254 days) with an average of 66 days.
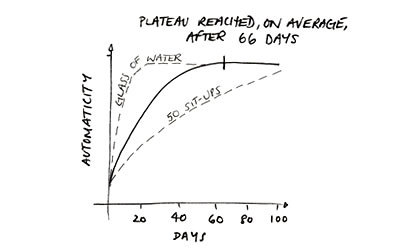
“When the researchers examined the different habits, many of the participants showed a curved relationship between practice and automaticity of the form depicted below (solid line). On average a plateau in automaticity was reached after 66 days. In other words it had become as much of a habit as it was ever going to become.” Source.
In a lot of ways, parenting becomes a habit. Mac and I take turns getting up in the night, and a lot of times, in the morning, we can’t remember how often or what time or for which kid. We’re on autopilot. On the rare occasion we are childless, we still go to open the rear car door to extract a small child or still tiptoe up the stairs at nap time.
I think this force of habit is what made the transition to motherhood so challenging with my first child, and much less so when adding a second. When transitioning to a new mom, I had to learn A LOT, adopt a whole new way of living, new skills, new routines, new patterns. When transitioning to a mom of two, all of that was old hat, there was just one extra kid to juggle.
So, to those expectant and new parents, hang in there. You can do it. Give it time. Cut yourself and each other lots of slack. This too shall pass. You’ll find your new normal.
What were your experiences becoming a new parent? Adding another child to your family? If you are expecting, what are you anticipating?
Read about the experiences of other evidence-based parents on School of Smock and follow our discussion on Twitter with the hashtag #parentscience and on our Facebook page.
Other posts I’ve done that might be useful for new and expecting parents:
My best parenting advice: Keep you expectations low
The Science of Breastfeeding (already a little out of date)
My experience with a C-section birth
Recovering from a repeat C-section (and some info on my recovery from the first) and here
Recovering from late onset, pregnancy-induced hypertension
Introducing potentially allergenic solids
Baby-led weaning, and here














